 |
synonyms: intersternocostoclavicular ossification, pustulotic arthroosteitis,
Sternoclavicular Hyperostosis ICD-9
Sternoclavicular Hyperostosis Etiology / Epidemiology / Natural History
- Soft-tissue ossification and hyperostosis between the clavicles, sternum and ribs
- Rare
- Generally males, bilateral. Patients age 30-50yrs old.
- More common in Japan.
- May also affect the anterior portions of the upper ribs and sternum, the distal femur and tibia, and the vertebral bodies
- Etiology unknown. Seronegative, HLA-B27 negative.
- Leads to severe shoulder ROM restrictions
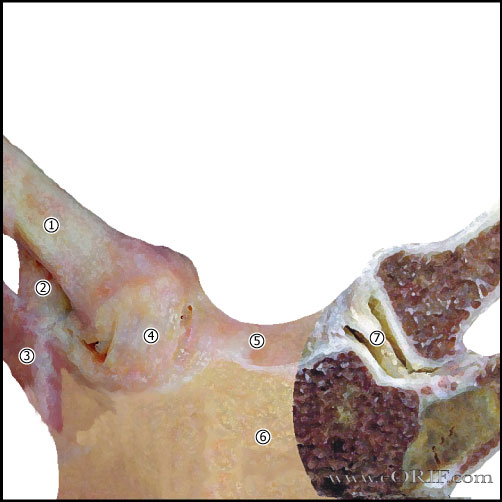
Sternoclavicular Hyperostosis Anatomy
- 50% of the medial head of the clavicle articulates with the sternum.
- SC joint allows 35° upward motion, 35° arc of A/P motion, 50° of rotation.
- SC joint is a diarthrodial joint.
- The only true articulation between the upper extremity and the axial skeleton.
- The medial clavicle epiphysis does not ossify until 17 or 18. In pts whose epiphysis is unossifed it is impossible to differential between a physeal fx and a dislocation, although fx is much more likely.
- Anterior capsular ligament is the strongest of the SC ligaments and prevents upward displacement of the medial clavicle.
- Costoclavicular ligament (rhomboid ligament): consists of anterior and posterior fasciculus. Anterior fasciculus arises from the anteriomedial aspect of the first rib and insert more laterally on the clavicle. Posterior fasciculus arises lateral to the anterior fasciculus and inserts more medially.
- Intra-articular Disk Ligament: dense, fibrous ligament arising from the synchondral junction of the first rib to the sternum; passes through the sternoclavicular joint, dividing it into two joint spaces.
- Interclavicular ligament: arises from the upper sternum, inserts on superomedial clavicle.
- Posterior capsule most important structure in AP stability of the medial clavicle.
- Safe resection length from the inferior articular surface of the medial clavicle to the most medial insertion of the costoclavicular ligament is 10 mm (Bisson LJ, JSES 2003;12:592).
Sternoclavicular Hyperostosis Clinical Evaluation
- Pain, swelling. warmth over the sternoclavicular joints and upper chest
- Advanced cases will have marked limitations in shoulder ROM.
Sternoclavicular Hyperostosis Xray / Diagnositc Tests
- AP view, apical lordotic view, serendipity view. Demonstrate hyperostosis of the sternum, clavicles, and upper ribs as well as ossification of the costoclavicular, costosternal, and intercostal ligaments (Davies AM, Skeletal Radiol 1999;28:159).
- CT scan is generally helpful. Demonstrates ossification of ligamentous structures around SC joint.
- Labs: ESR will be elevated. Other rheumatologic markers are normal.
- Biopsy: demonstrates chronic nonspecific inflammation and new bone formation.
Sternoclavicular Hyperostosis Classification / Treatment
- Staging (Sonozaki H, Arch Orthop Trauma Surg 1979;95:13).
- Stage I: mild ossification of the costoclavicular ligaments
- Stage II: ossific mass between the clavicle and first rib
- Stage III: bone mass between clavicle, sternum and 1st rib.
- Other manifestations: synovitis, hyperostosis, osteitis.
- Treatment = NSAIDs, activity modifications, may consider immunosuppressive therapy with cyclosporin A (rheumatology referral).
Sternoclavicular Hyperostosis Associated Injuries / Differential Diagnosis
Sternoclavicular Hyperostosis Complications
Sternoclavicular Hyperostosis Follow-up Care
- Generally followed by rheumatologist.
Sternoclavicular Hyperostosis Review References
- Kahn MF, J Rheumatol 1991;18:1104-1108.
- Higginbotham TO, JAAOS 2005;13:138
|