 |
synonyms: sternoclavicular infection, sternclavicular joint septic arthritis
Sternoclavicular Septic Arthritis ICD-9
Sternoclavicular Septic Arthritis Etiology / Epidemiology / Natural History
- Uncommon
- Risk factors: rheumatoid arthritis, sepsis, infected subclavian central lines, alcoholism, HIV/AIDs, renal dialysis, IV drug abuse, immunocompromise, diabetes mellitus
- Associated pathogens: Pseudomonas aeruginosa=intravenous drug abuse. Neisseria gonorrhoeae/Candida albicans=HIVpatients, Mycobacterium tuberculosis=immunocompromised patients or patients from 3rd world countries.
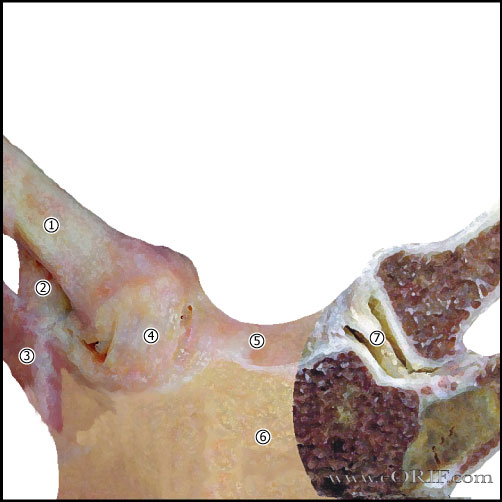
Sternoclavicular Septic Arthritis Anatomy
- 50% of the medial head of the clavicle articulates with the sternum.
- SC joint allows 35° upward motion, 35° arc of A/P motion, 50° of rotation.
- SC joint is a diarthrodial joint.
- The only true articulation between the upper extremity and the axial skeleton.
- The medial clavicle epiphysis does not ossify until 17 or 18. In pts whose epiphysis is unossifed it is impossible to differential between a physeal fx and a dislocation, although fx is much more likely.
- Anterior capsular ligament is the strongest of the SC ligaments and prevents upward displacement of the medial clavicle.
- Costoclavicular ligament (rhomboid ligament): consists of anterior and posterior fasciculus. Anterior fasciculus arises from the anteriomedial aspect of the first rib and insert more laterally on the clavicle. Posterior fasciculus arises lateral to the anterior fasciculus and inserts more medially.
- Intra-articular Disk Ligament: dense, fibrous ligament arising from the synchondral junction of the first rib to the sternum; passes through the sternoclavicular joint, dividing it into two joint spaces.
- Interclavicular ligament: arises from the upper sternum, inserts on superomedial clavicle.
- Posterior capsule most important structure in AP stability of the medial clavicle.
Sternoclavicular Septic Arthritis Clinical Evaluation
- SC joint pain, swelling, tenderness.
- Fever, chills, night sweats
Sternoclavicular Septic Arthritis Xray / Diagnositc Tests
- AP view, apical lordotic view, serendipity view. May demonstrate sclerosis, lytic or mixed lesions
- CT provides improved diagnostic value.
- MRI best delineates underlying abscesses.
- Labs: elevated ESR, CRP. WBC
- Diagnosis requires needle aspiration or biopsy for cultures and sensitivities.
- Historically unilateral enlargement of the sternoclavicular joint is a diagnositic sign of congenital syphilis
Sternoclavicular Septic Arthritis Classification / Treatment
- Irrigation and drainage with appropriate IV antibiotics.
- Consider sternoclavicular joint resection +/- resection of involved portions of the first and second ribs with appropriate soft-tissue coverage for failure to improve with I&D. (Song HK, Ann Thorac Surg 2002;73:427).
- Consider aspiration and IV antibiotics alone in previously healthy adults (Bar-Natan M, Semin Arthritis Rheum 2002;32:189).
Sternoclavicular Septic Arthritis Associated Injuries / Differential Diagnosis
Sternoclavicular Septic Arthritis Complications
- Cutaneous abcess
- Extrapleural abcess (Chen WS, JBJS 1993;75:1835).
- Intrathoracic abscess formation.
- Death (intrathoracic abscess formation with retrosternal vascular involvement).
Sternoclavicular Septic Arthritis Follow-up Care
Sternoclavicular Septic Arthritis Review References
|