|



|
synonyms: SC Dislocation, Medial Clavicle Dislocations, Clavicular physeal fracture, sternoclavicular dislocation
Sternoclavicular Dislocation ICD-10
A- initial encounter
D- subsequent encounter
S- sequela
Sternoclavicular Dislocation ICD-9
- 839.61(dislocation of sernum; sternoclavicular joint: closed)
- 839.71(dislocation of sernum; sternoclavicular joint: open)
Sternoclavicular Dislocation Etiology / Epidemiology / Natural History
- Require tremendous force, ie car accident, or fall, pile-on accident, trapped between two opposing forces.
- Generally results from indirect force when the shoulder is rolled forward during lateral compression producing a posterior SC dislocation or rolled backwards producing and anterior SC dislocation. May also occur from direct force on the anteromedial clavicle.
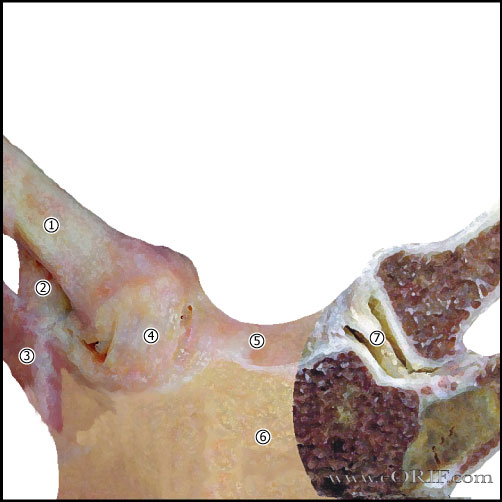
Sternoclavicular Dislocation Anatomy
- 50% of the medial head of the clavicle articulates with the sternum.
- SC joint allows 35° upward motion, 35° arc of A/P motion, 50° of rotation.
- SC joint is a diarthrodial joint.
- The only true articulation between the upper extremity and the axial skeleton.
- The medial clavicle epiphysis does not ossify until 17 or 18. In pts whose epiphysis is unossifed it is impossible to differential between a physeal fx and a dislocation, although fx is much more likely.
- Anterior capsular ligament is the strongest of the SC ligaments and prevents upward displacement of the medial clavicle.
- Costoclavicular ligament (rhomboid ligament): consists of anterior and posterior fasciculus. Anterior fasciculus arises from the anteriomedial aspect of the first rib and insert more laterally on the clavicle. Posterior fasciculus arises lateral to the anterior fasciculus and inserts more medially.
- Intra-articular Disk Ligament: dense, fibrous ligament arising from the synchondral junction of the first rib to the sternum; passes through the sternoclavicular joint, dividing it into two joint spaces.
- Interclavicular ligament: arises from the upper sternum, inserts on superomedial clavicle.
- Posterior capsule most important structure in AP stability of the medial clavicle.
Sternoclavicular Dislocation Clinical Evaluation
- Posterior dislocations generally have dysphagia, shortness of breath, pain in shoulder/medial clavicle and tendernesss.
- Anterior dislocation generally show visible, palpable displacement and tenderness.
- Neurvascular exam of the involved extremity indicated.
Sternoclavicular Dislocation Xray / Diagnositc Tests
- AP view, apical lordotic view, serendipity view
- Chest xray: If the injured medial clavicle is superior to the normal side the dislocation is anterior. If the injured medial clavicle is inferior to the normal side it is dislocated posteriorly.
- Serendipity View: 40-degree cephalic tilt a/p xray of SC joint. Draw a horizontal line across the image at the superior edge of the normal clavicular head. It the medial clavicle is superior to that line, it is dislocated anteriorly. If the medial clavicle is inferior, it is dislocated posteriorly.
- The medial clavicle epiphysis does not ossify until 17 or 18. In pts whose epiphysis is unossifed it is impossible to differential between a physeal fx and a dislocation, although fx is much more likely.
- CT scan is generally indicated. Assess whether dislocation is anterior or posterior, as well as injuries to associated vascular injuries / tracheal compression / impingement / hematoma.
Sternoclavicular Dislocation Classification / Treatment
- Posterior dislocation: closed reduction performed in OR with patient’s chest prepped and draped and CT surgeon on standby. Type and crossed blood available. Open reduction with costoclavicular and capsular ligament repair if fails closed reduction. Place folded towels/sandbag between scapulas. Pt supine on table. Apply traction to abducted arm in line with clavicle. Then slowly move arm into mild extension while gently pulling medial clavicle anteriorly. May consider using towel clip to aid in reduction. Closed reduction is typically difficult to maintain if >48hours since injury. If closed reduction is unsuccessful proceed with open reduction and Sternoclavicular Joint Reconstruction.
- Posterior physeal injury: closed reduction followed by sling and swathe. Consider open reduction if unable to reduce closed.
- Anterior physeal injury: symptomatic treatment without reduction. Physis will remodel with little to no functional limitations.
- Anterior dislocation: sling and swathe +/- closed reduction depending on amount of displacement.
- Chronic injuries are unlikely to be reduced closed due to soft tissue interposition/scar
- Never transfix SC joint with wires/pins as HW failure +/- pin migration into chest is the general rule with hardware in the SC joint due to tremendous lever arm on SC joint.
- See also Sternoclavicular Joint Reconstruction Technique.
Sternoclavicular Dislocation Associated Injuries / Differential Diagnosis
Sternoclavicular Dislocation Complications
- Pneumothorax
- Laceration of superior vena cava, pulmonary artery
- Brachial plexus injury
- Rupture of the aorta or esophagus
- Shortness of breath
- Hoarseness
- Difficulty swallowing
- Thoracic outlet syndrome
Sternoclavicular Dislocation Follow-up Care
- Figure of eight brace with sling for 4-6 wks. Obtain follow-up radiographs.
- 6 Weeks: begin gentle ROM exercises with gradual return to activities.
Sternoclavicular Dislocation Review References
|

