|



|
synonyms: glenoid fracture scapula fracture shoulder joint fracture
Glenoid Fracture ICD-10
- S42.141A - Displaced fracture of glenoid cavity of scapula, right shoulder, initial encounter for closed fracture
- S42.142A - Displaced fracture of glenoid cavity of scapula, left shoulder, initial encounter for closed fracture
- S42.143A - Displaced fracture of glenoid cavity of scapula, unspecified shoulder, initial encounter for closed fracture
- S42.144A - Nondisplaced fracture of glenoid cavity of scapula, right shoulder, initial encounter for closed fracture
- S42.145A - Nondisplaced fracture of glenoid cavity of scapula, left shoulder, initial encounter for closed fracture
- S42.146A - Nondisplaced fracture of glenoid cavity of scapula, unspecified shoulder, initial encounter for closed fracture
- See all Glenoid fracture ICD-10 codes.
A - initial encounter for closed fracture
B - initial encounter for open fracture
D - subsequent encounter for fracture with routine healing
G - subsequent encounter for fracture with delayed healing
K - subsequent encounter for fracture with nonunion
P - subsequent encounter for fracture with malunion
S - sequela
Glenoid Fracture ICD-9
- 811.03 (fracture of scapula, closed, glenoid cavity and neck of scapula)
Glenoid Fracture Etiology / Epidemiology / Natural History
- Include fractures of the glenoid rim and glenoid fossa.
- Result from impaction of the humeral head against the glenoid from medially directed forces.
Glenoid Fracture Anatomy
Glenoid Fracture Clinical Evaluation
- These are typically high enegery injuries, assessment should begins with the A,B,C's.
- C/O shoulder pain after trauma. Shoulder often held in abduction and external rotation
- Evaluate for tenderness, ecchymosis, soft tissue injury.
- Document axillary, median, ulnar, radial nerve function and radial pulse.
Glenoid Fracture Xray / Diagnositc Tests
- AP, scapular lateral and axillary views.
- CT scan with 2-3mm cuts often helpful to fully define fracture pattern.
- Consider Chest xray to rule out associated injuries.
Glenoid Fracture Classification / Treatment
- Nondisplaced / minimally displaced : immobilization in a sling for 1 wk followed by progressive ROM and physical therapy.
- Displaced (subluxation of humeral head, >10mm displacement, >1/4 of glenoid cavity anteriorly or >1/3 of the glenoid cavity posteriorly, >5mm articular step-off): ORIF (Kavanaugh BF, JBJS 1993;75A:479).
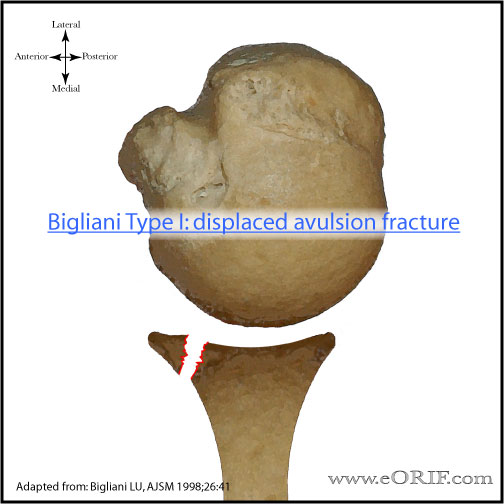
- Idelberg Classification: Type I:glenoid rim, Type II:superior 30-50% of the glenoid surface with the coracoid, Types III, IV, V: involve lateral border of the scapula, Type VI:severely comminuted.
Glenoid Fracture Technique
- Contraindications: severely comminunted fractures which preclude satisfactory fixation.
- Most glenoid fractures are approached posteriorly.
- Anterior Rim fractures = anterior approach-exposure of the lateral border of the scapula is limited by axillary nerve and posterior humeral circumflex vessles that cross the proximal portion of the lateral scapule(inferior glenoid) to reach the quadrangular space.
- It is important to review scapular anatomy before surgery. Look at a skeleton and review areas in which fixation can be placed in the scapula.
- Consent for iliac crest bone graft if needed.
- Pre-op antibiotics, SCD's on bilateral lower extremities
- General endotracheal anesthesia
- Folley catheter
- Lateral decubitus position; axillary role; pad all bony prominences
- Prep and drap in standard sterile fashion
- Incision over lateral spine of the scapula alone posterior aspect of acromion.
- Expose posterior deltoid and subperiosteally reflect it off its origin from the scapular spine and acromion. This exposes the underlying infraspinatus and teres minor.
- Incise inferior 1/2 of the infraspinatus insertion and open the interval between the infraspinatus and teres minor. This exposes posterior capsule.
- Infraspinatus is reflect of the caspule and retracted superiorly.
- Posterior capsule is incised from the humerus and elcvated superiorly exposing the glenoid. Fukuda retractor can be used to hold humeral head anteriorly.
- Fracture is identified, reduced and fixed using standard AO techniques. Fixation is generally provided with 3.5mm reconstruction plates, and / or 3.5mm or 4.0mm cannulated screws.
- Keep in mind the majority of the scapula is paper thin. Adequate bone stock to hold screws can be found: in the glenoid neck, coracoid process, base of the scapular spine, and lateral border of the scapular body.
- Irrigate
- Close in layers
Glenoid Fracture Associated Injuries / Differential Diagnosis
- >80% incidence of associated injury
- Rib fracture, pulmonary contusion, pneumothorax, pulmonary contusion, spinal cord injury
- Brachial Plexus palsy
- Clavicle Fracture
- Proximal Humerus Fracture
- Scapular Fracture
- Acromioclavicular dislocation
- Sternoclavicular dislocation
- Scapulthoracic dissociation
- Coracoid Fracture
- Glenohumeral instability
- Floating Shoulder
Glenoid Fracture Complications
- Heterotopic Ossification
- Nerve injury: axillary
- Glenohumeral arthritis
- Nonunion
- Malunion
- Infection
- Stiffness
Glenoid Fracture Follow-up Care
- Shoulder immobilizer with gentle pendulum, elbow/wrist/hand ROM immediately
- F/U at 7-10 days. Start physcial therapy for gentle ROM exercises at first post-op visit.
- ROM and strengthening are advanced dependent on fracture type, fixation and healing. Generally patients remain in the sling for 6 weeks. Has limited use of the extremiity for 10-12 weeks and must refrain from heavy physical activity for 4-6 months.
- 89% good/excellent outcomes with ORIF of displaced fractures (Kavanaugh BF, JBJS 1993;75A:479).
- Shoulder Outcome Measures.
Glenoid Fracture Review References
|