|



|
synonyms: long head of biceps tendon rupture, biceps tendon tear
Proximal Biceps Rupture ICD-9
- 727.62(rupture of long head of biceps tendon, nontraumatic)
Proximal Biceps Rupture Etiology / Epidemiology / Natural History
- May occur from inflammatory arthritis, osteoarthritis, osteochondromatosis, osteophyte in bicipital groove (usually medial wall), rotator cuff pathology, biceps instability
- Has been reported in softball players, weightlifters (Cope MR, JSES 2004;13:580) and baseball players.
- Nonsurgical treatment leads to 21% deficit in suppination, 8% deficit in elbow flexion strength, but no weakness in grip, pronation, or elbow extension and infrequent pain. (Mariani E, CORR 1988;288:233).
- Long head of biceps tendon subluxation/dislocation/rupture occurs in 31%-56% of isolated subscap tears (Deautsch A, AJSM 1997;25:13), (Gerber C, JBJS 1996;78A:1015)
-
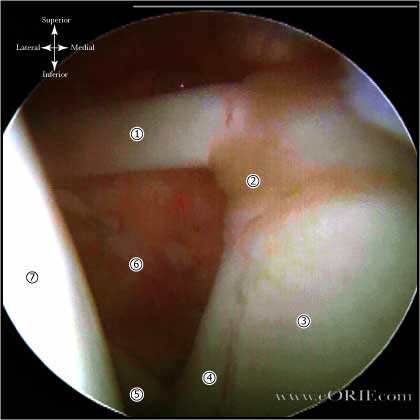
Proximal Biceps Rupture Anatomy
- Long head of the biceps tendon functions as a humeral head depressor and is a secondary restraint to anterior instability, particularily in the abducted/internally rotated position (Kumar VP CORR 1989:244:172)
- Stabilizing ligamentous pulley of the biceps consists of the confluence of the superior glenohumeral ligament and the coracohumeral ligament with fibrous contributions from the subscapularis and supraspinatus tendons. (Bennett WF, Arthroscopy 2001;17:173).
- Intra-articular rupture of the biceps tendon is associated with subscapularis rupture.
- see also Shoulder Anatomy.
Proximal Biceps Rupture Clinical Evaluation
- Painless deformity of the arm with biceps retracted distally into a ball (Popeye sign). Acute ruptures may have localized swelling and ecchymosis.
- Yergusons:
- Speed's:
- Cross-body adduction causes anterior shoulder pain instead of AC joint pain
- Impingement signs may be postive
- Normal active/passive shoulder ROM.
Proximal Biceps Rupture Xray / Diagnositc Tests
- AP, scapular lateral and axillary views: generally normal.
- MRI (+/- arthrogram) demonstrates ruptured long head of biceps tendon retracted into bicipital groove, as well as associated pathology ( RTC tear).
Proximal Biceps Rupture Classification / Treatment
- Acute, young physcially active patient: Biceps tenodesis.
- Acute, elderly low demand patient: rest, ice, NSAIDs, gentle ROM as tolerated. Return to activities including sports as symptoms allow. Generally avoid heavy lifting for 3 months.
- Chronic: generally treated non-operatively unless significant cosmetic concerns arise.
- Most biceps lesions are associated with other inciting pathology which should be corrected at the time of surgery.
- AAOS handout.
Proximal Biceps Rupture Tenodesis
- CPT: 23430 (tenodesis of long tendon of biceps)
- Indicated for younger, more physically active patients
- arthroscopic tenodesis with absorbable interference screw (Boileau Arthroscopy 2002:18:1002-1012) Technique
- Percutaneous Intra-articular Trans-tendon technique: (Sekiya JK, Arthroscopy 2003;19:1137). Easily performed and does not require any supplemental hardware.
- 30 degrees flexion, 30 degrees IR, 30 degrees abduction. Elbow flexed to 90 degrees.
Proximal Biceps Rupture Associated Injuries / Differential Diagnosis
Proximal Biceps Rupture Complications
- Cosmetic deformity
- Pain
- Weakness
Proximal Biceps Rupture Follow-up Care
- Non-operatively treated patients gradually improve over 2-3 months with limited if any functional or strengths deficients. Cosmetic deformity with the biceps muscle belly rolled up into distal arm may develop, but is generally asymptomatic.
- Biceps tenodisis patients are protect with a posterior splint or sling for weeks with immediate passive elbow and shoulder ROM. Muscle strengthening is started at 6 weeks. Return to sporting activites at 3-6 months.
Proximal Biceps Rupture Review References
|