|

|
synonyms: cervical angina
Cervical Radiculopathy ICD-10
Cervical Radiculopathy ICD-9
- 723.4 Brachia neuritis or radiculitis; cervical radiculitis, radicular symdrome of upper limbs.
Cervical Radiculopathy Etiology / Epidemiology / Natural History
- Definition: pain in a radicular pattern in one or both upper extremities related to compression and/or irritation of one or more cervical nerve roots. Frequent signs and symptoms include varying degrees of sensory, motor and reflex changes as well as dysesthesias and paresthesias related to nerve root(s) without evidence of spinal cord dysfunction (myelopathy). (NASS 2010 Guideline)
- Natural History has not been conclusively determined. The symptoms are often self-limited and resolve spontaneously without specific treatment. Symptom length is variable.
- Commonly caused by disc herniation and spondylosis.
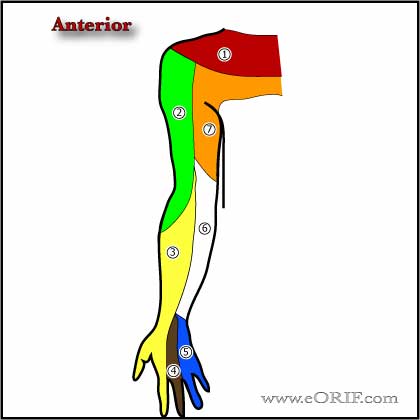
Cervical Radiculopathy Anatomy
- Symptoms are produced in the root exiting at the level of pathlogy. Example: C6 root symptoms from C5-6 herniation.
Cervical Radiculopathy Clinical Evaluation
- Arm pain (99.4%), neck pain (79.7%), scapular pain (52.5%), anterior chest pain (17.8%) and headache (9.7%). (Henderson CM, Neurosurgery. 1983;13:504)
- Pain / paresthesia in a dermatomal pattern (53.9%), diffuse/nondermatomal pattern (45.5%)
- Sensory change to pinprick (85.2%) , motor deficit (68%), decrease in a DTR (71.2%).
- Cervical angina = left chest and arm pain
- Neck, shoulder, arm pain, paresthesias and numbness in a dermatomal distribution weakness in a myotomal distributionn, +/- occipital headache
- Atypical findings such as deltoid weakness, scapular winging, weakness of the intrinsic muscles of the hand, chest or deep breast pain, headaches
- Spurling’s test positive(increased symptoms with rotation and lateral bend with a vetical compressive force)
- Abduction relief sign: relief of pain when the arm is placed overhead.
- C2: extremely rare-jaw pain and occipital headaches, but no motor deficit is seen.
- C3: most often caused by disk disease at C2-3, is not common-headaches and pain along the posterior aspect of the neck that extends tothe posterior occipital region and occasionally to the ear. There are no motor deficits,. DDX:tension headaches.
- C4: typically C3-4 HNP-posterior neck and trapezial pain, decreased sensation in C4 dermatome, no motor deficits, and diaphragmatic involvement has not been well documented. Patients occasionally complain of numbness and pain at the base of the neck that extends to the shoulder and scapular region.
- C5: pain and/or numbness in an “epaulet” pattern that includes the superior aspect of the shoulders (suprascapular) and the lateral aspect of the upper arm. Deltoid motor function is often weakened, as in an intrinsic shoulder disorder; the diagnosis of radiculopathy at this site is crystallized by observing the absence of impingement signs or pain with passive shoulder motion. Patients may complain of difficulties with activities of daily living if there is involvement of the supraspinatus, infraspinatus, or elbow flexors. Depression of the biceps reflex is an inconsistent finding.
- C6: pain or sensory abnormalities extending from the neck to the biceps region, down the lateral aspect of the forearm to the dorsal surface of the hand, between the thumb and index finger, and including the tips of these fingers. May have suprascapular shoulder pain. The brachioradialis reflex may be depressed, and wrist extensor weakness is usually present. The infraspinatus, serratus anterior, triceps, supinator, and extensor pollicis muscles may also be affected.
- C7: most common. Pain and sensory abnormalities extend down the posterior aspect of the arm and the posterolateral aspect of the forearm and typically involve the middle finger, which is rarely affected in C6 disorders. May have interscapular shoulder pain. Absence of the triceps reflex is common, and triceps weakness is almost always present. The wrist flexors, wrist pronators, finger extensors, and latissimus dorsi may also be affected. May have scapular winging.
- C8: least likely to be associated with pain, but may have interscapular or scapular shoulder pain. Sensory changes usually restricted to below the wrist; interossei motor involvement. DDX: ulnar neuropathies, intrinsic hand disorders, myelopathy.
- Long Track signs indicate myelopathy
-Babinski's Reflex: upturning and splaying of the toes with plantar stimulus
-Hoffman's sign: flexion of the thumb and index fingers in response to flicking the tip of the outstretched middle finger
-Lhermitte's sign: shooting sensations down the arm with rapid neck flexion.
-Clonus
Cervical Radiculopathy Xray / Diagnositc Tests
- Xray Indications: trauma, systemic disease(RA), cancer, pain for >6weeks, night pain, neuroligc findings. Xrays are oftern not indicated initially.
- A/P, Lateral, Odontoid, flexion / extention lateral views. Evaluated for instability, pseudarthrosis, atlantoaxial arthrosis. Typically shows loss of disk height, end-plate osteophytosis, malaignment. A/P vew may demonstrate uncovertebral DJD or scoliosis
- CT: useful for fracture, foraminal stenosis, facet arthropathy.
- MRI: demonstrates disc degeneration, neruologic compression, infection, tumor.
- Facet injections: helpful to diagnosis facet mediated pain.
- EMG/NCV.
Cervical Radiculopathy Classification / Treatment
- Non-op treatment= traction, physcial therapeutic exercise, traction, NSAIDs, patient education (Saal, Spine 21:1877, 1996).
- Surgical:
-Laminoforaminotomy: Indicated for foraminal stenosis or lateral to foraminal disk herniations without significant neck pain or instability. posterior approach, remove lateral edge of superior and inferior lamina and dorsal aspect of exiting neuroforamen, remove disc fragments. If >50% of facet is removed consider fusion. (Adamson TE, J Neurosurg 2001;95suppl 1:51).
-ACDF (anterior diskectomy and fusion): Indicated for spondylosis and/or central or paracentral disc pathology. (Bohlman HH, JBJS 1993;75A:1298).
- Total disk replacement: long term outcomes unknown.
Cervical Radiculopathy Associated Injuries / Differential Diagnosis
- Carpal tunnel syndrome
- Cubital tunnel syndrome
- Thoracic outlet syndrome
- Myelopathy
- Cauda Equina Syndrome
- Ulnar tunnel syndrome
- RTC tear
- Subacromial Impingement
Cervical Radiculopathy Complications
- Recurrent laryngeal nerve palsy (more common with right sided anterior approaches)
- Horner's syndrome (sympathetic chain neuropraxia)
- Dysphagia
- Dysphonia
- Vertebral artery injury
- Pseudoarthrosis
- Adjacent segment degeneration: 2.9%/yr (Hilibrand AS, JBJS 1999;81A:519).
Cervical Radiculopathy Follow-up Care
Cervical Radiculopathy Review References
- NASS Evidence-Based Clinical Guideline: Diagnosis and Treatment of Cervical Radiculopathy from Degenerative Disorders. 2010
- °
|
