|

|
synonyms: stingers, pinch-stretch brachial plexus neuropraxia, burners syndrome
Burner Syndrome ICD-10
Burner Syndrome Etiology / Epidemiology / Natural History
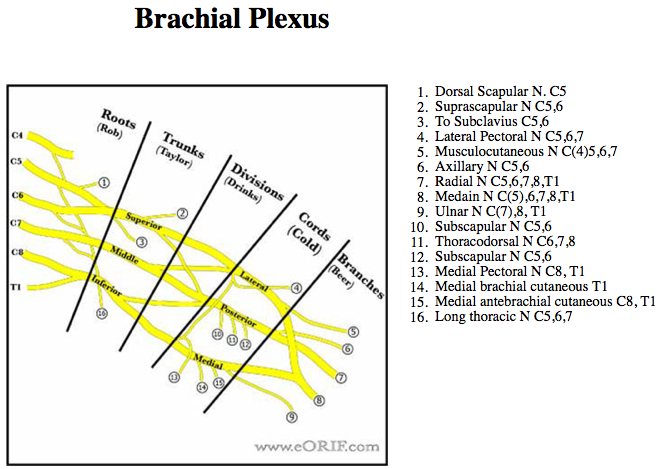
- Thought to be related to brachial plexus stretch and/or nerve root compression. Generally involves the upper trunk of the bracial plexus, particularily C5-C6.
- Typically traction injury with axial distraction or downward force on the shoulder and coexistent lateral bend of the neck away from the shoulder.
- Brachial plexus stretch injuries: young athletes, neck pain less common.
- Nerve root compression: older athletes (college), generally associated with cervical disc disease or cervical stenosis. Neck pain more common.
Burner Syndrome Anatomy
- Generally involves upper trunk of brachail plexus; C5 nerve root.
- 93% of football players with chronic stingers have significant disk disease or neural foraminal narrowing. (Levitz CL,AJSM 1997;25(1): 73-76)
Burner Syndrome Clinical Evaluation
- Unilateral sharp burning pain in the neck +/- radiation into the shoulder and down the arm after a blunt force to the head/neck/shoulder.
- Generally caused by lateral neck flexion away from the involved area and shoulder depression on the involved side.
- May have associated weakness in shoulder abduction, elbow flexion and external rotation.
- Full-pain free neck ROM.
- Spurling's test: passive extension and lateral flexion of the head and neck reproduces symptoms / pain. Associated with nerve root compression.
- Bilateral symptoms indicate cervical neuropraxia, not Burners syndrome. (Torg JS, Sports Med 1995;20:429).
Burner Syndrome Xray / Diagnositc Tests
- Cervical spine xrays indicated if neck pain is present. Patients with abnormal xrays including cervical stenosis(developmental or degenerative), loss of lordosis, foraminal narrowing and degenerative changes are at increased risk of cervical spine trauma. Patients witha Torg ratio <0.8 may not participate in contact sports.
- Consider EMG/NCV if weakness persists for greater than 4 weeks. EMG changes typically continue after clinical recovery. Abnormal EMG findings do not preclude sports participation.
- MRI: indicated for patients with bilateral symptoms (cervical neuropraxia).
Burner Syndrome Classification / Treatment
- Return to play: allowed if paresthesias completely abates, full muscle strength is restored and patient has full, pain-free cervical ROM. Patients with bilateral symptoms (cervical neurapraxia) may not return to play until cleared by cervical MRI. Patients found to have Cervical Spinal Stenosis 723.0 may not play in contact sports.
- 3 or more stingers in a season: consider no return to sport for season; Xrays, MRI.
- Patients witha Torg ratio <0.8 have Cervical Spinal Stenosis 723.0 and are at increased risk of cervical spine injury and may not play contact sports.
- Persistent Symptoms: continued paresthesia, weakness, limitation cervical motion, recurrent episodes; xray / MRI / EMG indicated before return to sport.
- Prophylaxis: neck and shoulder strengthening, Cowboy Collar
 / high-profile shoulder pads. Equipement has not been clinical demonstrated to prevent recurrence. / high-profile shoulder pads. Equipement has not been clinical demonstrated to prevent recurrence.
- Seddon Classification of Nerve Injury.
Burner Syndrome Associated Injuries / Differential Diagnosis
Burner Syndrome Complications
- Permanent muscle atrophy, sensory loss
Burner Syndrome Follow-up Care
- May return to play if paresthesias completel abates, full muscle strength is restored and patient has full, pain-free cervical ROM.
- Prevention of recurrence is based on aggressive neck and shoulder strengthening. Neck rolls, cowboy colars and high-profile shoulder pads are also advisable.
Burner Syndrome Review References
- Fogel GR, JAAOS 2004;12:49
- Torg JS, AJSM 1990;18:50.
- Torg JS, Sports Med 1995;20:429
- Kelly JD IV, Am J Sports Med 2000;28:214
- Thomas BE, JAAOS 1999;7:333
|