|

Otto-Bock
Ossur Rheo
|
Amputation ICD-10 Codes
|
Acquired Absense ICD-10 codes
Z89.011 Right thumb
Z89.012 Left thumb
Z89.021 Right finger(s)
Z89.022 Left finger(s)
Z89.111 Right hand
Z89.112 Left hand
Z89.121 Right wrist
Z89.122 Left wrist
Z89.211 Right upper limb below elbow
Z89.212 Left upper limb below elbow
Z89.221 Right upper limb above elbow
Z89.222 Left upper limb above elbow
Z89.231 Right shoulder
Z89.232 Left shoulder
|
Z89.411 Right great toe
Z89.412 Left great toe
Z89.421 Right other toe(s)
Z89.422 Left other toe(s)
Z89.431 Right foot
Z89.432 Left foot
Z89.441 Right ankle
Z89.442 Left ankle
Z89.511 Right leg below knee
Z89.512 Left leg below knee
Z89.521 Right knee
Z89.522 Left knee
Z89.611 Right leg above knee
Z89.612 Left leg above knee
Z89.621 Right hip joint
Z89.622 Left hip joint
|
Indications
- Traumatic amputation
- unrepairable vascular injury
- Mangled extremity
- Septic extremity
- Residual limb less functional than prosthesis
- Type III-C open tibial fractures with disruption of the tibial nerve or a crush injury with warm ischemia time > 6 hours.
- Widespread necrosis in medically unstable patient
- Severe open tibial fracture with crushed foot.
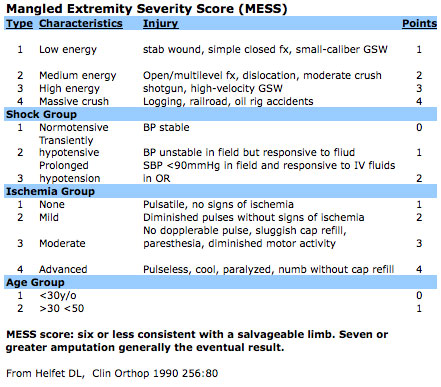
- Amputation predictors: mangled extremity severity score (MESS); NISSSA (nerve injury, ischemia, soft- tissue injury, skeletal injury, shock , age); Predictive Salvage Index (PSI); Limb Salvage Index (LSI). All have low sensitivity, high specificity and are not generally recommended as a criterion for amputation. (Bosse MJ, JBJS, 2001;83A:3).
- MESS score: six or less consistent with a salvageable limb. Seven or greater amputation generally the eventual result.
Considerations
- Amputation should be performed at the most distal level possible to improve ability to ambulate, decrease energy cost of walking and improve function.
- Pre-operative aids in determining amputation level: skin color, hair growth, and skin temperature, Transcutaneous oxygen tension (40 mmHg indicates good healing potential; if <40mmHg but >20mmHg consider elevating the extremity for 3 minutes, a decrease of >15mmHg indicates poor healing potential.
- Malnourished(serum albumin < 3.5 g/dl, total lymphocyte level < 1500cells/ml) or immunocompromised patients have markedly increased rates of perioperative complications.
Complications
- 69% phantom limb pain (Gallagher P Disabil Rehabil 2001;23:522)
- 42% residual limb pain
- 50% painful neuroma (consider gabapentin, pregabalin)
Post-Op Management
- 3 weeks: remove sutures, start shrinker sock
- 6 weeks: casting for socket/prosthesis fabrication
- 8 weeks: start therapy once patient is able to done prosthesis and stand for 15 minutes. 4-8 weeks of therapy.
- Consider gabapentin, pregabalin for limb pain / neuroma
Scapulothoracic / Forequarter Amputation
- Nerves: brachial plexus
- Vessels: subclavian artery and vein
- Concerns: Semi lateral postion, remove entire scapula, most of clavicle.
Shoulder Disarticulation
- Nerves: brachial plexus.
- Vessels: cephalic vein, brachial vessels/axillary artery, thoracoacromial artery
- Concerns: modified shoulder disartic with small portion of proximal humerus remaining is best (cut at surgical neck). Use deltoid myofasciocutaneous flap advanced distally to cover axilla. Reattach pec major and latissimus dorsi to humeral head, leave RTC intact.
Trans-Humeral (Above Elbow)
- Nerves:Median N, Radial N, Ulnar N
- Vessels: brachial artery, profunda brachii artery, cephalic vein, basilic vein
- Concerns: Equal anterior and posterior skin flaps. Length=1/2 the diameter of the arm. Generally utilize posterior triceps flap for distal bone coverage. Biceps and triceps are myodesed via bone tunnels. Level of bone section should be at lease 3.8cm proximal to the elbow joint to allow room for the elbow-lock mechanism of the prosthesis.
Elbow Disarticulation
- Nerves:ulnar nerve, median nerve, radial nerve
- Vessels: cephalic vein, brachial vein, brachial artery, basilic vein, radial recurrent artery and vein
- Concerns: anterior flap should extend just distal to the radial tuberosity. Posterior flap should extend 2.5cm distal to tip of olecranon. Suture ticeps the biceps and brachialis. Preserve 6cm of extensor muscle mass to suture into the medial epicondyle.
Trans-Radial (Below Elbow amputation, BEA, forearm amputation)
- Nerves: anterior interosseous N, superficial branch of radial nerve, posterior interosseous N, ulnar nerve, median N
- Vessels: anterior inteosseous artery, radial artery, ulnar artery, basilic vein, cephalic vein.
- Concerns: 4-5cm of proximal ulna needed. Equal anterior and posterior flaps. Length = slightly longer than 1/2 the forearm diameter. Consider creating an anterior flap of flexor digitorum sublimis sutured into the deep dorsal fascia. Never use the entire anterior muscle mass.
Wrist Disarticulation
- Nerves:Ulnar nerve, Median Nerve, Superficial branch of radial nerve, dorsal branch of nerve
- Vessels: radial artery, unlar artery
- Concerns: preserving the distal radioulnar joint preserves suppination and pronation ability. Fish mouth incision with larger palmar flap. Allow resected tendons to retract into forearm. Countour radial and ulnar styoids to smooth surface.
Hip Disarticulation
- Nerves: femoral nerve,
- Vessels: femoral artery and vein
- Concerns: posterior flap with raquet-shaped incision.
Trans-Femoral Amputations (above knee, AKA)
- Nerves/Vessels: (1)deep femoral artery / 2 veins (2)Sciatic nerve follow branches up to it:tibial nerve, peroneal nerve, sural nerve ?obturator nerve, great saphenous vein, superficial femoral artery / vein?
- Concerns: preserve adductors and abductors for balance;
- Equal anterior and posterior flaps with lengths = 1/2 diameter of the limb +1cm
- Ideal Stump length: preserve 50%-50% of femoral length. Leaving less than 2 inches of femur functions as hip disarticulation, but with complicated prosthesis fitting. At least 3 inches of femur must be removed for socket, adaptors and connections to the prosthetic knee. If less than 2 inches of femur remaining consider hip disarticulation.
- ASEC technique and video.
Knee Disarticulation
- Nerves/Vessels: (1)saphenous N & greater saphenous vein (2) tibial N, popliteal artery and vein (3) common peroneal N (4) sural N, small saphenous vein.
- Concerns: Retain gastroc and cruciates. Generally posterior flap, can do sagittal flaps.
- Posterior flap length = diameter of the leg at the femoral condyles + 1cm.
- Best option for non-ambulatory patients. Transtibial amputation has increased risk of wound problems and knee flexion contractures. Transfemoral amputation has shorter lever arm which decreases bed mobility, transfer ability and sitting stability.
- Descreased walking energy expenditure compared to transfemoral amputation. better thigh muscle balance, increased prosthesis stability. Fewer knee-joint prosthetic components, poor cosmesis compared to transfemoral prosthesis.
- ASEC technique and video.
- (Bowker JH, JBJS 2000;82A:1571), (Mazet R JR, JBJS 1966;48A:126)
Trans-Tibial Amputations (below knee, BKA)
|

{kind=link}